WASHINGTON — Lone neutrons quickly decay, but scientists don’t agree on how long the particles stick around before their demise. New experiments could resolve the dispute — or deepen the mystery.
Outside of a nucleus, neutrons survive only about 15 minutes on average. They quickly decay into a proton, an electron and an antineutrino. Two methods used for measuring the neutron lifetime disagree, leaving scientists uncertain about the subatomic particle’s true longevity (SN: 5/19/12, p. 20). One technique involves containing chilled neutrons in a trap, or “bottle,” waiting awhile, and counting the remaining neutrons to determine how many decayed. Other experiments monitor beams of neutrons and count the number of decays by detecting the protons emitted. Bottle measurements come up with lifetimes about 9 seconds shorter than beam measurements.
“This is actually fairly important for a number of things,” physicist Robert Pattie said January 29 at a meeting of the American Physical Society. In particular, pinning down the neutron’s lifetime is necessary for understanding how atomic nuclei began forming after the Big Bang. Scientists’ befuddlement makes it harder to calculate the properties of the early universe.
One drawback of typical bottle experiments is that neutrons can be absorbed or otherwise lost when they hit the wall of the bottle. So Pattie, of the Los Alamos National Laboratory in New Mexico, and colleagues are working on an updated bottle-style measurement using a magnetic field to keep neutrons from hitting the bottom of the trap, while gravity keeps them from flying out of the top.
Physicist Craig Huffer of North Carolina State University in Raleigh and colleagues are working on a bottle experiment that uses a magnetic field to trap neutrons. Rather than counting neutrons at the end, the researchers detect flashes of light produced as neutrons inside the bottle decay away.
In beam experiments, accuracy depends on making a careful count of the neutrons beamed in and the protons produced in the decays, physicist Shannon Fogwell Hoogerheide of the National Institute of Standards and Technology in Gaithersburg, Md., explained at the meeting on January 30. She and colleagues are refining their beam measurement to better enumerate protons and neutrons. Some scientists have suggested the discrepancy could have deeper meaning. The short lifetime in bottle measurements could indicate that neutrons are somehow disappearing unexpectedly, making the lifetime appear shorter than it really is. “Kind of an out-there mechanism is that they’ve gone into some kind of alternative reality, which we call the mirror world,” says physicist Ben Rybolt of the University of Tennessee. In such a world, all the particles we know of would be duplicated — mirror protons, neutrons and electrons could exist, which would interact only very slightly with the particles we know.
Jumping to such an explanation for the neutron lifetime discrepancy is “a little bit of a leap,” Rybolt acknowledges, but such mirror particles could also explain the conundrum of dark matter, an unseen substance indicated by the motions of stars inside galaxies. To test the idea, Rybolt and colleagues are proposing to shoot beams of neutrons at a barrier and check if any make it through, which could indicate the particles had briefly become mirror neutrons.
The problem of measuring the neutron’s lifetime is complex enough that a variety of new techniques are under preparation to unravel the issue. “I don’t think one additional experiment can resolve the discrepancy,” says Huffer. Instead, multiple new measurements with different techniques should eventually converge on the correct value.
Almost every night that the constellation Orion is visible, physicist Mark Vagins steps outside to peer at a reddish star at the right shoulder of the mythical figure. “You can see the color of Betelgeuse with the naked eye. It’s very striking, this red, red star,” he says. “It may not be in my lifetime, but one of these days, that star is going to explode.”
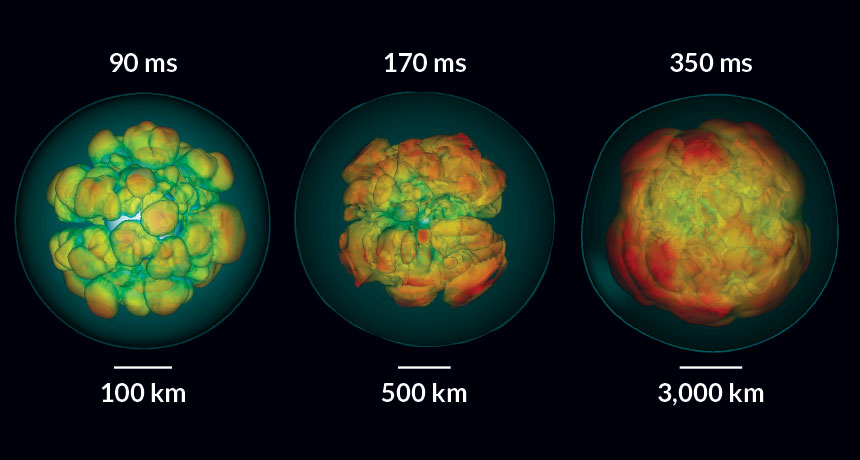
With a radius about 900 times that of the sun, Betelgeuse is a monstrous star that is nearing its end. Eventually, it will no longer be able to support its own weight, and its core will collapse. A shock wave from that collapse will speed outward, violently expelling the star’s outer layers in a massive explosion known as a supernova. When Betelgeuse detonates, its cosmic kaboom will create a light show brighter than the full moon, visible even during the daytime. It could happen tomorrow, or a million years from now. Countless stars like Betelgeuse — any of which could soon explode — litter the Milky Way. Scientists estimate that a supernova occurs in our galaxy a few times a century. While brilliantly gleaming supernovas in far-flung galaxies are regularly spotted with telescopes trained on the heavens, scientists eagerly hope to capture two elusive signatures that are detectable only from a supernova closer to home. These signatures are neutrinos (subatomic particles that stream out of a collapsing star’s center) and gravitational waves (subtle vibrations of spacetime that will also ripple out from the convulsing star). “These two signals, directly from the interior of the supernova, are the ones we are really longing for,” says Hans-Thomas Janka, an astrophysicist at the Max Planck Institute for Astrophysics in Garching, Germany. Unlike light, which is released from the star’s surface, stealthy neutrinos and gravitational waves would give scientists a glimpse of the processes that occur deep inside a collapsing star.
Supernovas offer more than awe-inspiring explosions. When they erupt, the stars spew out their guts, seeding the cosmos with chemical elements necessary for life to exist. “We clearly wouldn’t be here without supernovas,” says Vagins, of the Kavli Institute for the Physics and Mathematics of the Universe at the University of Tokyo. But the processes that occur within the churning mess are still not fully understood. Computer simulations have revealed much of the physics of how stars explode, but models are no substitute for a real-life nearby blast.
One inspiration for scientists is supernova 1987A, which appeared in the Large Magellanic Cloud, a satellite galaxy of the Milky Way, 30 years ago (SN: 2/18/17, p. 20). That flare-up hinted at the unparalleled information nearby supernovas could provide. With the detectors available at the time, scientists managed to nab just two dozen of 1987A’s neutrinos (SN: 3/21/87, p. 180). Hundreds of papers have been written analyzing that precious handful of particles. Calculations based on those detections confirmed scientists’ hunch that unfathomably large numbers of neutrinos are released after a star’s core collapses in a supernova. In total, 1987A emitted about 1058 neutrinos. To put that in perspective, there are about 1024 stars in the observable universe — a vastly smaller number.
Since 1987, neutrino detectors have proliferated, installed in exotic locales that are ideal for neutrino snagging, from the Antarctic ice sheet to deep mines across the globe. If a supernova went off in the Milky Way today, scientists could potentially nab thousands or even a million neutrinos. Gravitational wave detection has likewise come on the scene, ready to pick up a slight shift in spacetime stirred up by the blast. Detecting such gravitational waves or a surfeit of supernova neutrinos would lead to a distinct leap in scientists’ knowledge, and provide new windows into supernovas. All that’s needed now is the explosion.
Early warning Despite estimates that a few stars explode in the Milky Way every century, no one has glimpsed one since the early 1600s. It’s possible the explosions have simply gone unnoticed, says physicist John Beacom of Ohio State University in Columbus; light can be lost in the mess of gas and dust in the galaxy. A burst of neutrinos from a supernova would provide a surefire signal.
These hermitlike elementary particles shun most interactions with matter. Produced in stars, radioactive decay and other reactions, neutrinos are so intangible that trillions of neutrinos from 1987A’s explosion passed through the body of every human on Earth, yet nobody felt a thing. For supernovas like 1987A, known as type 2 or core-collapse supernovas, about 99 percent of the explosion’s energy goes into the tiny particles. Another, less common kind of supernova, type 1a, occurs when a remnant of a star called a white dwarf steals matter from a companion star until the white dwarf explodes (SN: 4/30/16, p. 20). In type 1a supernovas, there’s no core collapse, so neutrinos from these explosions are much less numerous and are less likely to be detectable on Earth.
For scientists studying supernovas, neutrinos’ reluctance to interact is an advantage. The particles don’t get bogged down in their exit from the star, so they arrive at Earth several hours or even more than a day before light from the explosion, which is released only after the shock wave travels from the star’s core up to its surface. That means the particles can tip off astronomers that a light burst is imminent, and potentially where it is going to occur, so they can have their telescopes ready.
Most neutrino experiments (there are more than a dozen) weren’t built for the purpose of taking snapshots of unpredictable supernovas; they were built to study neutrinos from reliable sources, like the sun, nuclear reactors or particle accelerators. Nevertheless, seven neutrino experiments have joined forces to create the SuperNova Early Warning System, SNEWS. If neutrino detectors in at least two locations report an unexpectedly large burst of neutrinos, SNEWS will send an e-mail alert to the world’s astronomers. The experiments involved are a weirdly diverse bunch, including IceCube, a detector composed of light sensors frozen deep in the ice of Antarctica (SN: 12/27/14, p. 27); Super-Kamiokande, which boasts a tank filled with 50,000 tons of water stationed in a mine in Hida, Japan; and the Helium and Lead Observatory, or HALO — with the motto “astronomically patient” — made of salvaged lead blocks in a mine in Sudbury, Canada. Their common thread: The experiments are big to provide a lot of material for neutrinos to interact with — such as lead, water or ice.
With light sensors sunk kilometers deep into the ice sheet, IceCube’s detector is so huge that it could pick up traces of a million neutrinos from a Milky Way supernova. Because it was designed to capture only the highest energy neutrinos that are rocketing through space, it’s not sensitive enough to detect individual neutrinos emitted during a supernova. Instead, IceCube’s focus is on the big picture: It catalogs an increase of light in its detectors produced by neutrinos interacting in the ice in time slices of two billionths of a second, says IceCube leader Francis Halzen of the University of Wisconsin–Madison. “We make a movie of the supernova.”
Super-Kamiokande is the neutrino detector that can pinpoint the location of the impending stellar paroxysm. It is a successor to Kamiokande-II, one of a few detectors to spot a handful of neutrinos from 1987A. Shortly after a burst of neutrinos from a nearby supernova, the detector could direct astronomers to zero in on a few degrees of sky. If that happens, says neutrino physicist Kate Scholberg of Duke University, “I expect anybody with the capability will be zooming in.” On the lookout Various neutrino detectors await signals emitted from a supernova, including Super-Kamiokande in Japan, IceCube in Antarctica and HALO in Canada. They are joined by a gravitational wave observatory, LIGO, with detectors in Louisiana (shown) and Washington state.
Languages of a supernova Light and neutrinos are two of several languages that a supernova speaks. In that sense, supernova 1987A was a “Rosetta stone,” Beacom says. By scrutinizing 1987A’s light and its handful of neutrinos, scientists began piecing together the theoretical physics that explains what happened inside the star. In a future supernova, another language, gravitational waves, could add nuance to the tale. But the explosion has got to be close.
If neutrinos are elusive, gravitational waves border on undetectable. Minute tremors in space itself, predicted by Einstein’s general theory of relativity, are generated when massive objects accelerate. In 2016, scientists with the Advanced Laser Interferometer Gravitational-Wave Observatory, LIGO, announced the first direct detection of gravitational waves, produced by two merging black holes (SN: 3/5/16, p. 6). That milestone required a pair of detectors so precise that they can sense quivers that squish the detectors’ 4-kilometer-long arms by just a tiny fraction of the diameter of a proton.
Gravitational waves from a supernova should be even harder to tease out than those from merging black holes. The pattern of ripples is less predictable. Surveys of the properties of the many supernovas detected in other galaxies indicate that the explosions vary significantly from one to the next, says astroparticle physicist Shunsaku Horiuchi of Virginia Tech in Blacksburg. “We ask, ‘Is there a standard supernova?’ The answer is ‘No.’ ”
Despite the challenges, finding gravitational waves from supernovas is a possibility because the explosions are chaotic and asymmetrical, producing lumpy, lopsided bursts. An explosion that expands perfectly symmetrically, like an inflating balloon, would produce no gravitational waves. The gravitational wave signature thus can tell scientists how cockeyed the detonation was and how fast the star was spinning.
Gravitational waves might also reveal some of the physics of the strange stew of neutrons that makes up a protoneutron star — the beginnings of an incredibly dense star formed in a supernova. Scientists would like to catalog the compressibility of the neutron-rich material — how it gets squeezed and rebounds in the collapse. “The gravitational wave signature would have an imprint in it of this stiffness or softness,” says computational astrophysicist Tony Mezzacappa of the University of Tennessee.
There’s a chance the supernova would collapse into an even more enigmatic state — a black hole, which has a gravitational field so strong that not even light can escape. When a black hole forms, the flow of neutrinos would abruptly drop, as their exit route is cut off. Detectors would notice. “Seeing the moment that a black hole is born,” says Vagins, “would be a tremendously exciting thing.”
While neutrinos can be oracles of supernovas, a stellar explosion could reveal a lot about neutrinos themselves. There are three types of neutrinos: electron, muon and tau. All are extremely light, with masses less than a millionth that of an electron (SN: 1/26/13, p. 18). But scientists don’t know which of the three neutrinos is the lightest; a nearby supernova could answer that question.
Supernovas, with all the obscure physics at their hearts, have a direct connection to Earth. They are a source of many of the elements from which planets eventually form. As stars age, they fuse together heavier and heavier elements, forging helium from hydrogen, carbon from helium and so on up the periodic table to iron. Those elements, including some considered essential to life, such as carbon and oxygen, spew out from a star’s innards in the explosion.
“All the elements that exist — that are here on Earth — that are heavier than iron were either made in supernovas or other cataclysmic events in astronomy,” says physicist Clarence Virtue of Laurentian University in Sudbury, Canada. Gold, platinum and many other elements heavier than iron are produced in a chain of reactions in which neutrons are rapidly absorbed, known as the r-process (SN: 5/14/16, p. 9). But scientists still argue about whether the r-process occurs in supernovas or when neutron stars merge with one another. Pulling back the curtain on supernovas could help scientists resolve the dispute.
Even the reason supernovas explode and sow their chemical seeds has been vigorously debated. Until recently, computer simulations of supernovas have often fizzled, indicating that something happens in a real explosion that scientists are missing. The shock wave seems to need an extra kick to make it out of the star and produce the luminous explosion. The most recent simulations indicate that the additional oomph is most likely imparted by neutrinos streaming outward. But, says Mezzacappa, “At the end of the day, we’re going to need some observations against which we can check our models.”
Hurry up and wait Supernovas’ potential to answer such big questions means that scientists are under pressure not to miss a big break. “You better be ready. If it happens and you’re not ready, then you will be sad,” Scholberg says. “We have to be as prepared as possible to gather as much information as we possibly can.” If a detector isn’t operating at the crucial moment, there’s no second chance. So neutrino experiments are designed to run with little downtime and to skirt potential failure modes — a sudden flood of data from a supernova could crash electronics systems in an ultrasensitive detector, for example. Gravitational wave detectors are so finicky that interference as subtle as waves crashing on a nearby beach can throw them out of whack. And in upcoming years, LIGO is scheduled to have detectors off for months at a time for upgrades. Scientists can only hope that, when a supernova comes, everything is up and running.
Some even hope that neighboring stars hold off a little longer. “It seems like I’m always telling people that I’d like Betelgeuse to go off one year from now,” jokes Bronson Messer, a physicist who works on supernova simulations at Oak Ridge National Laboratory in Tennessee. With each improvement of the simulations, he’s eager for a bit more time to study them.
Messer keeps getting his wish, but he doesn’t want to wait too long. He’d like to see a supernova in the Milky Way during his lifetime. But it could be many decades. Just in case, Vagins, who’s been taking those nightly peeks at Betelgeuse, is doing his part to prepare the next generation. He no longer scans the skies alone. “I’ve already taught my 6-year-old son how to find that star in the sky,” he says. “Maybe I won’t get to see it go, but maybe he’ll get to see it go.”
NASA’s Juno spacecraft will stay in its current 53-day orbit around Jupiter instead of closing into a 14-day orbit as originally planned, the Juno team announced February 17.
An issue with two helium check valves, which are tied to the spacecraft’s main engine, had scientists concerned. The valves took several minutes to open when the team pressurized the spacecraft’s propulsion system in October. During previous main engine firings, the valves took only a few seconds to open.
Another main engine burn to put the spacecraft into a shorter orbit poses a risk to completing the science goals of the mission, mission scientists say.
Juno has been circling Jupiter since July 4. Staying in the longer orbit will not change the date of the next flyby, nor will it affect voting for which Jovian features to be imaged with JunoCam. It will allow the team to probe Jupiter’s magnetic field in more depth than originally planned. And it may also help to maintain the health of the spacecraft because Juno will spend less time exposed to the planet’s radiation belts, the team noted.
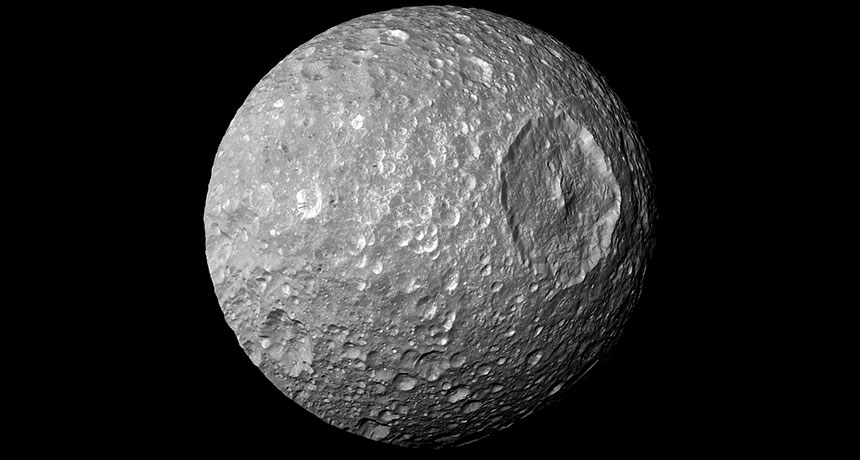
An ocean of liquid water probably doesn’t lurk beneath the icy surface of Mimas, Saturn’s smallest major moon, new calculations suggest. In 2014, scientists had proposed the ocean to help explain an odd wobble in the moon’s orbit (SN: 11/15/14, p. 16).
Other ocean-harboring moons, such as Jupiter’s Europa and Saturn’s Enceladus, are crisscrossed by fractures opened by strong tides that cause their oceans to bulge outward. Mimas, though freckled with craters, lacks any such cracks.
Planetary scientist Alyssa Rhoden of Arizona State University in Tempe and colleagues calculated whether Mimas’ icy shell could withstand the stress of a subsurface ocean pushing outward. Taking into account the moon’s elongated orbit, the team estimates that a subsurface ocean would produce tidal stresses larger than those on crack-riddled Europa. Mimas therefore probably doesn’t have an ocean, the researchers conclude February 24 in the Journal of Geophysical Research: Planets.
As the planet warms, carbon stashed in Earth’s soils could escape into the atmosphere far faster than previously thought. In the worst-case scenario for climate change, carbon dioxide emissions from soil-dwelling microbes could increase by 34 to 37 percent by 2100, researchers report online March 9 in Science. Previous studies predicted a more modest 9 to 12 percent rise if no efforts are taken to curb climate change. Those extra emissions could further intensify global warming.
Much of that extra CO2 will originate from soils at depths overlooked by previous measurements, says study coauthor Margaret Torn, a biogeochemist at Lawrence Berkeley National Laboratory in California. “We ignore the deep at our peril,” she says. Soils cover about two-thirds of Earth’s ice-free land area and store nearly 3 trillion metric tons of organic carbon — more than three times the amount of carbon in the atmosphere. Dead organisms such as plants contribute to this carbon stockpile, and carbon-munching microbes belch some of that carbon into the atmosphere as CO2. Rising temperatures will spur the microbes to speed up their plant consumption, scientists warn, releasing more CO2 into the air. And the data back up that fear.
Scientists have mimicked future warming by heating the top 5 to 20 centimeters of experimental soil plots and measuring the resulting CO2 emissions. Those studies missed deeper soils, though, known to contain more than half of all soil carbon. Warming such deep soils is technically challenging and scientists had generally assumed that any emission increases from so far down were insignificant, says study coauthor Caitlin Hicks Pries, an ecosystem ecologist at Lawrence Berkeley.
Using heating coils and rods embedded in the soil, Hicks Pries, Torn and colleagues warmed a plot of soil for over two years in the forested foothills of California’s Sierra Nevada. The warmth extended to a meter below ground, the full depth of the soil in the area. That heating replicated the roughly 4 degrees Celsius of warming expected by the end of the century in a worst-case scenario. Annual carbon emissions from the soil jumped from 1,100 grams per square meter to 1,450 grams per square meter. Around 40 percent of this emissions increase originated below a depth of 15 centimeters, with 10 percent originating below 30 centimeters.
Assuming other soils behave similarly, by 2100, the increase in the CO2 emission rate from just the soils deeper than 30 centimeters could equal modern-day CO2 emission rates from oil burning, the researchers estimate.
While only 13.5 percent of Earth’s soils resemble the woodland soils examined in the study, Torn says that the experiment shows that scientists need to consider deep soils when calculating future climate change. Studies already in the works will test if the results hold true for other soil types.
The new experiment is exciting and well executed, says Katherine Todd-Brown, a biogeochemist at the Pacific Northwest National Laboratory in Richland, Wash. The net impact soils will have on future climate change, however, remains unclear, she says. The amount of carbon from the atmosphere entering soils could also increase as higher CO2 concentrations and warmer environments promote plant growth. That increased carbon drawdown could offset the climate impacts of the increased emissions, though the magnitude of that effect is still debated (SN Online: 9/22/16). “You really have to take both the inputs and outputs into account,” Todd-Brown says.
Grasses have top-notch border control to conserve water in their leaves. Now, scientists have identified the genetic switch that makes them such masters at taking in carbon dioxide without losing water. The find might eventually help scientists create more drought-resistant crop plants, the researchers report in the March 17 Science.
Adjustable pores called stomata on the undersides of leaves help plants take in CO2 while minimizing water loss. Like pupils responding to sunlight, plants open and close their stomata in response to changing light, humidity and temperature. Grass stomata can open wider and respond more quickly than those in other plants, which helps grasses photosynthesize more efficiently. This ability might help explain why grasses grow successfully in so many places on Earth, says Brent Helliker, a plant ecologist at the University of Pennsylvania who wasn’t part of the new study. For instance, grasses are particularly well equipped to deal with the rapidly changing weather and strong winds that can hit plains and prairies.
In most plant stomata, two kidney bean–shaped cells, one on each side of the pore, swell or deflate like balloons to control the size of the opening. But in grass, each of these cells is shaped like a dumbbell instead. And each dumbbell is linked to two other cells called subsidiary cells. Scientists have long suspected that grasses’ subsidiary cells might give the dumbbells, known as guard cells, an assist by making it easier for them to open and close. But that’s been hard to test in a controlled way. When a stoma opens, “it’s elbowing its way into the neighbor cells,” says study coauthor Dominique Bergmann, a biologist at Stanford University. “If the neighbors don’t want to move, you’re stuck.” But subsidiary cells have some squish. As guard cells inflate, their neighboring subsidiary cells deflate. Bergmann and her colleagues mutated a gene called MUTE in purple false brome (Brachypodium distachyon) so that the grass didn’t make the MUTE protein. Without MUTE, plants didn’t make subsidiary cells. And without the helping hand, the plants were less efficient than usual at opening and closing their stomata.
Grasses aren’t the only plants that have the MUTE gene, Bergmann says. But in other plants, the gene provides instructions to help make guard cells, not subsidiary cells. At some point in grasses’ evolution, the MUTE gene took on a function that differs from the rest of the plant kingdom.
Although the new work confirms that subsidiary cells and guard cells work together to make grass stomata more responsive, more research is still needed to understand exactly how subsidiary cells lend a hand. “It would be really nice to show that there’s actually an exchange of ions between the two cell types,” says Michael Blatt, a plant physiologist at the University of Glasgow in Scotland. Sharing ions could incentivize water to flow from one cell type to the other, controlling which one is more inflated.
More responsive stomata may have helped grasses survive during periods when Earth’s climate was warm and dry. “Grasses got lucky,” says study coauthor Michael Raissig, also at Stanford. As Earth’s climate continues to change, Raissig says, these genetic innovations might be exploited to help other plants make it through, too.
Dengue is a bit of a homebody. By mapping the spread of the virus across Bangkok, scientists found that infections were most likely to occur within a few minutes’ walk of the home of the first person infected.
Pinpointing where dengue is likely to be transmitted can better focus efforts to stop the spread of the disease, the researchers report in the March 24 Science.
“We often think of transmission and infection as occurring in this ubiquitous, pervasive and amorphous way,” says study coauthor Derek Cummings. But there is a pattern to how dengue spreads. This study, he adds, shows that scientists are “starting to have the tools and methods to really track how infectious diseases move across a population.” Dengue is a viral disease transmitted by Aedes aegypti mosquitoes and can cause fever and muscle pain so excruciating that it’s also known as “breakbone fever.” In some cases, it can be deadly, resulting in more than 20,000 deaths per year. Cummings and colleagues looked at both the genetics and locations of about 18,000 cases of dengue from 1994 to 2010 in Thailand, most from the capital Bangkok. If two cases of dengue evolved from the same parent strain of the virus within a season, or about six months, researchers considered the pair to belong to the same transmission chain, which connects dengue infections that spread from one person to the next. About 160 chains occur in Bangkok in a season.
The researchers found that 60 percent of dengue cases within a 200-meter radius in Bangkok were closely related. These infections with a particular dengue strain belonged to the same transmission chain, says Cummings, an epidemiologist at the University of Florida in Gainesville. In contrast, only three percent of cases separated by a greater distance, between one to five kilometers, were from the same transmission chain. The new study’s combination of genetic and location information provides more details on the ecology of dengue than previous research, says Caroline Buckee, an infectious disease epidemiologist at the Harvard School of Public Health. “It would be great to see this kind of approach become a standard for studies of dengue transmission and epidemiology.”
When the researchers mapped the locations of cases within the same transmission chain, they found that the home of the person originally infected by a mosquito bite, the first link in the chain, is a good indicator of where new cases of dengue will occur.
Thailand’s Ministry of Public Health responds to dengue infections by spraying to kill mosquitoes. “Now, we have some quantitative details to start targeting control technologies,” Cummings says, to better focus spraying in high-priority areas.
The data may also be helpful for a vaccine. Though there is a dengue vaccine licensed for use in Thailand, Cummings says, researchers don’t know yet whether the vaccine will need to be updated with more strains of the virus over time, like the flu shot. Understanding the diversity of dengue strains and how they spread across Bangkok in a season may help researchers address this vaccine concern, he adds.
“Once we can understand these detailed patterns of how things spread, then we might be able to refine how we respond to the pathogen,” Cummings says.
In a spaceflight first, the aerospace company SpaceX has successfully launched and landed a previously used rocket.
The Falcon 9 rocket blasted off March 30 from NASA’s Kennedy Space Flight Center in Florida at 6:27 p.m. EDT carrying a commercial telecommunications satellite. After separating from the rest of the rocket and its payload, the refurbished first stage of the rocket touched back down smoothly on a platform in the Atlantic Ocean. The stage is the same one SpaceX used in its first successful landing on an ocean barge in April 2016.
Although the aerospace company has recovered eight Falcon 9 rockets after previous launches, this homecoming marks the first time it has reflown one of those used boosters. In September, a Falcon 9 rocket and its payload exploded on the launchpad at Cape Canaveral during a routine test.
In the past, the spent first stages of rockets have been lost to the ocean. Capturing and reusing rockets may lead to cheaper spaceflights, the company says.
The pill is a sledgehammer approach to contraception…. A second-generation of [drugs] is being designed to do the job without upsetting a woman’s normal cycle of ovulation and menstruation…. A contraceptive administered to the man can be given only for a short time without actually affecting the development of sperm … and, therefore, is not being considered for actual clinical use. —Science News, April 15, 1967
Update Contraceptives have come a long way since 1967. Women can choose low-dose pills, hormonal rings, implants and intrauterine devices — effective methods that can be less disruptive to normal menstrual cycles. Men have far fewer options, but that may eventually change. A long-acting gel injected into 16 adult male rhesus monkeys’ reproductive tracts completely prevented pregnancy in their partners over one to two breeding periods. The gel works like a vasectomy but is less invasive and can be reversed more easily, researchers report February 7 in Basic and Clinical Andrology.
When I was pregnant, my pronoun shifted automatically. My “I” turned into “we,” as in, “What are we going to eat for dinner?” and, “Should we sit in that hot tub?” I thought about that shift to the majestic plural as we got our Tdap shot in our third trimester.
The Tdap vaccine protects against tetanus, diphtheria and pertussis, or whooping cough. Doctors recommend that women receive a dose with each pregnancy because the diseases can be particularly dangerous for young babies. But good, hard evidence for the benefits of vaccinating women while pregnant instead of shortly after giving birth has been lacking. A new study of nearly 150,000 newborns fills that gap for whooping cough.
Researchers at the Kaiser Permanente Vaccine Study Center in Oakland, Calif., studied the medical records of mothers who gave birth to babies between 2010 and 2015. Overall, about 46 percent of the mothers received a Tdap vaccine at least 8 days before giving birth.
Seventeen of the 150,000 babies got whooping cough by the time they were 2 months old. Of these 17 babies, only one had been born to a mother who had received the Tdap vaccine during her pregnancy. And this baby, the researchers note, had a mild case of whooping cough and wasn’t admitted to the hospital.
The maternal protection against whooping cough stuck around beyond 2 months, the researchers found. Though babies got their own vaccines in their first year of life, those babies who got their mothers’ antibodies during pregnancy were less likely to get whooping cough before their first birthdays than babies whose mothers had not been vaccinated while pregnant.
Babies whose mothers were vaccinated after giving birth didn’t get similar protection. The researchers found no evidence that postpartum Tdap vaccinations for mothers prevented whooping cough in babies. “Our results demonstrate the substantial benefit of vaccinating during pregnancy rather than waiting until after birth,” pediatrician and vaccine researcher Nicola Klein and colleagues wrote online April 3 in Pediatrics.
Since 2013, doctors have recommended that women get Tdap shots during every pregnancy between weeks 27 and 36 of pregnancy, a window that’s thought to be prime for antibody sharing. Babies usually get their first vaccine against whooping cough at 2 months of age. The new study shows how antibodies received in utero from mom can shepherd babies through this vulnerable unvaccinated period.
These days, whooping cough is making a comeback. That reemergence comes in part from a switch in the 1990s to a vaccine that comes with fewer side effects but is less effective. Changes in the bacterial culprit itself and lower vaccination rates also contribute to whooping cough’s reemergence. One of the best things mothers-to-be can do to keep their newborns healthy, the study shows, is to themselves deliver those antibodies to their babies by getting vaccinated during pregnancy.